In the United States, approximately 3%-5% of people over the age of 65 have severe aortic stenosis (AS), which, if left untreated, is associated with only a 50% chance of survival over three to five years due to the development of heart failure and sudden death. Survival is notably worse when patients begin having symptoms of fatigue, shortness of breath, chest discomfort, lightheadedness or syncope. Therefore, it has become standard of care to replace the aortic valve with surgical aortic valve replacement (SAVR) or transcatheter aortic valve replacement (TAVR) when symptoms develop. Replacing the severely stenotic aortic valve in symptomatic patients has proven to improve their survival as well as quality of life, with relief of symptoms. However, it is unknown whether asymptomatic patients with severe aortic stenosis would benefit from aortic valve replacement, as their prognosis is not as poor as those patients with symptoms and procedures such as SAVR and TAVR have a small risk of significant complications, including an approximate 1% chance of death and 1% chance of stroke.
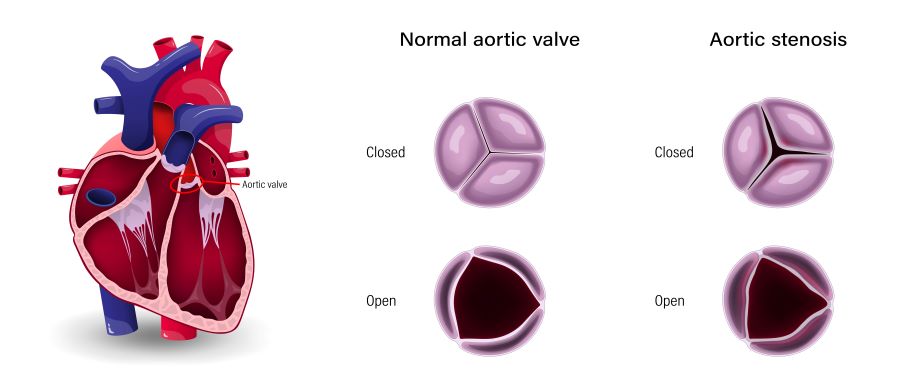
The EARLY TAVR trial has shown that TAVR is safe in patients with severe AS without symptoms and appears to reduce severe events, including the combined endpoints of hospitalization, stroke and death. It is important to note that there are different asymptomatic, severe aortic stenosis grades. Generally, the lower the aortic valve area and the greater the pressure gradient across the aortic valve, the worse the prognosis is for the patient. Patients who have very severe/critical AS or have evidence of heart failure on physical exam or worsening left ventricular function on an echocardiogram are already recommended aortic valve replacement, per national guidelines. Part of the problem with basing the decision to replace the aortic valve on symptoms alone is that many patients do not notice their symptoms because they have adapted to the disease by slowing down, refraining from activities that cause symptoms, or may feel that they’re just “getting older.”
Therefore, close follow-up with their cardiologist every three to six months and supplementary testing, such as exercise treadmill testing or checking the B-type natriuretic peptide (BNP) level, which increases in patients with subclinical heart failure, may lead to recommendations for aortic valve replacement sooner rather than later. The findings of the EARLY TAVR study are very encouraging in that they demonstrate the safety and efficacy of TAVR in these patients and will lead to closer monitoring of patients, with a low threshold to replace the aortic valve, even when patients do not disclose any symptoms.
Learn more about Northside Hospital Heart Institute.
